Basal Cell
Carcinoma.
BCC is the most common type of skin cancer.

BCC is the most common type of skin cancer.
BCC is a very common finding at a routine skin check.
This Skin cancer is classified as a ‘basaloid epithelial tumour’, which means that the cancerous cells arise from the basal layer of the epidermis. A pathologist can determine whether the growth is a BCC, although expert mole scanning has >90% accuracy in detecting BCCs.
The good news is that BCCs grow slowly and rarely spread to other parts of the body.
The downside of BCC is that it’s most commonly treated with surgery. Patients who are prone to multiple BCCs may have to undergo regular surgery.
BCC is ubiquitous in Australia. UV light is the major risk factor for BCC (primarily UVB). Intermittent intense exposure to sunlight is important, as well as long term cumulative sun exposure. The use of tanning machines greatly increases the risk.
Genes are an all-important risk factor for the development of BCC.
Interestingly, emerging evidence suggests that BCC is more common in people with lower Body Mass Index. This is because estrogen increases with higher body weight, and estrogen is thought to protect against BCC.
Immunosuppression is a strong risk factor for BCC, with a tenfold increase on the trunk and arms after a solid organ transplant. Another common risk factor is prior radiotherapy.
Rare risk factors are arsenic exposure and some hereditary conditions such as nevoid basal cell carcinoma syndrome.
Different types of BCC require different treatments. The broad category of BCC may be established clinically prior to excision. However, a pathology report is necessary to identify any concerning features and determine the subtype of BCC.
BCC subtypes include
Let’s look at these types of BCC in more detail.
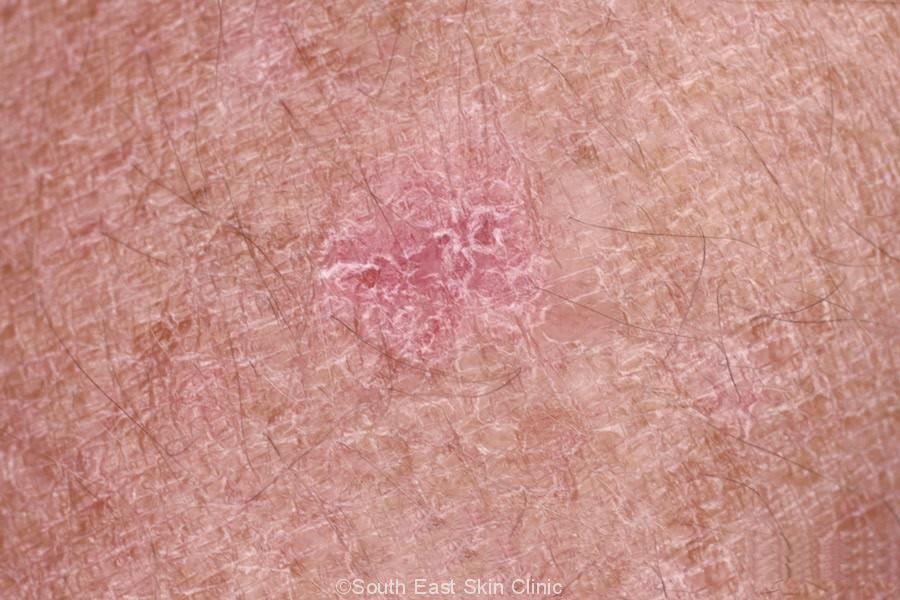
Superficial BCC accounts for around 30% of Basal Cell Carcinoma. The condition tends to occur in a younger age group than those affected by other BCC types. Genes play an important role in the development of superficial BCC.
Superficial BCC appears as a pink or red flat lesion with well-defined borders. Look for a subtly elevated and/or pearly edge that is best seen on stretching the skin. The lesion may be slightly shiny and/or scaly. Superficial BCC may look similar to an IEC (Bowen’s disease). A dermatoscope will certainly help distinguish the two with at least 90% accuracy.
Superficial BCC may be treated non-surgically. The most common non-surgical treatment is with Imiquimod (®Aldara) cream.
Gallery of Superficial BCC
Please click on the images for details.
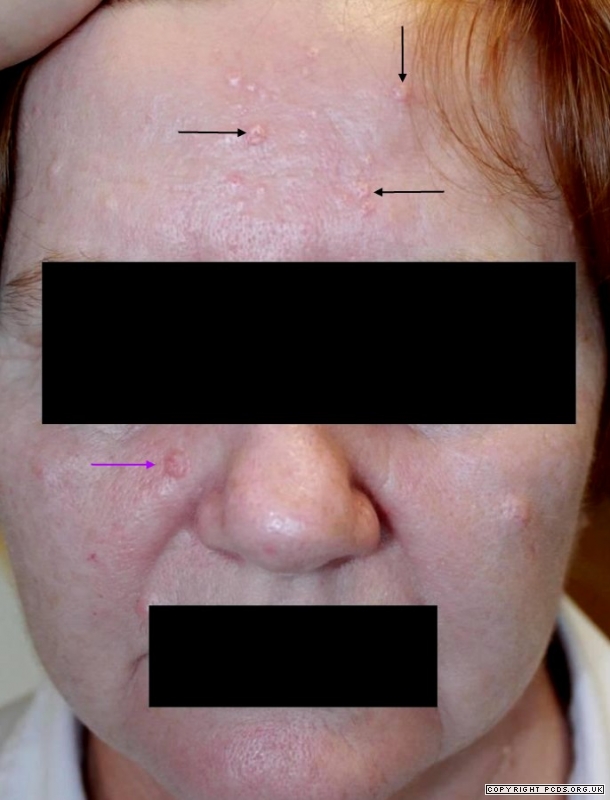
Nodular BCC is the most common type of BCC, accounting for around 60% of all Basal Cell Carcinoma. Nodular BCC is found most commonly on the face, head and neck.
A nodular BCC is a raised lesion, typically pink or red in colour. As with other types of BCCs, stretching the skin can bring out the pearly edge more clearly. There may be a central ulcer (the so-called ‘rodent ulcer’) or a central crust. Look for fine blood vessels connecting to a common vessel. These ‘Arborising Vessels’ are much better seen with a dermatoscope. The lesion may be itchy and tends to bleed with minor scratching.
Gallery of Nodular BCC
Please click on the images for details.
A Pigmented BCC is simply that … a BCC with pigment! This type of BCC accounts for approximately 8% of BCC and is more common in people with darker skin types. Pigmented BCC is not usually completely pigmented and will have some pink to red areas. The BCC may be flat (‘superficial’) or raised (‘nodular’). The appearance of deeply pigmented BCC is quite similar to that of melanoma.
Gallery of Pigmented BCC
Please click on the images for details.
Morphoeic Basal Cell Carcinoma accounts for 5 to 10% of BCC. ‘Morphoeic’ refers to the scar-like appearance.
The features of Morpheic BCC are:
A morphoeic BCC is harder to treat than other types of BCC.
Gallery of Morphoeic BCC
Please click on the images for details.
SURGERY FOR BCC
Surgery is the most effective treatment for BCC. The risk of a BCC coming back after surgery is increased with:
Surgical margins are generally wider for a BCC with any of these risk factors.
Let’s illustrate the scar size with numbers. Take a small BCC that is just 4mm in diameter. The BCC is cut out with 3mm margins, resulting in a scar that is 24mm long. Now take a 6mm BCC. The scar is now 30mm long. In fact, for every extra 1 mm in diameter, the scar will be 3-4mm longer. This is clearly an issue on the face or scalp where a skin graft or flap may be required. Bear in mind that these figures are conservative, and some types of BCC will need a wider excision.
BCC may need to be cut out with much wider margins that you think.
TOPICAL TREATMENT OF BCC
The ‘aggressive types’ of BCC are usually treated with surgery.
Superficial BCC may be treated topically.
The number one topical treatment is ©Aldara cream, although fluorouracil 5% cream and PDT are occasionally used.
©Aldara cream is the branded version of Imiquimod cream and works by stimulating the immune system to get rid of the cancer cells.
The cream is in the region of 80% to 85% effective.
A starting-point treatment regime is 5 overnight applications per week for 6 weeks. The cream will make the skin red and inflamed. You actually want a good reaction for the cream to work. However, a severe reaction could leave the skin with permanent loss or increase of pigment. Your doctor will carefully advise you on how to use the cream and may advise a week’s break if the reaction is too severe. Treating wider areas can result in flu-type symptoms.
As a result of all of this, surgery may appear to be a better alternative than six weeks of inflamed, itchy, and/or sore skin – particularly when considering the higher rate of recurrence after topical treatment.
For patients prone to many BCCs, non-surgical treatments without biopsy are a viable option – there are pros and cons to this approach, but a subset of patients can benefit from this strategy.
SKIN SURVEILLANCE
A person with a previous BCC has a 17-fold increased risk of a new BCC relative to someone who has not had a previous BCC. There is a 2-fold increased risk of melanoma and a 3-fold increased risk of Squamous Cell Carcinoma (SCC).
A new BCC will form in just under half of people diagnosed with a BCC in the last 2 years
More frequent skin cancer examinations will be required, and regular self-examinations are also helpful.
What are the BCC subtypes that are shown on the Pathology Report?
The clinical types of BCC have already been described above: superficial (flat), nodular (raised), pigmented, and Morphoeic (scar-like).
Pathology reports may not match clinical types of BCC, and certain types can only be identified on the basis of the pathology report.
It is important to know which type of BCC you have from the pathology report because some require additional treatment or monitoring.
BCC pathology reports will often include the term ‘palisading’, and this refers to BCC cells that clump together as blocks or rows along the edge of the BCC.
Perineural invasion is the invasion of nerves by the tumour and, though not common, indicates a more aggressive cancer.
Superficial BCC
Very common type of BCC that corresponds to the pre-excision clinical superficial BCC.
The BCC cells are arranged horizontally in the upper part of the dermis (papillary dermis) and the epidermis. The BCC does not spread deeply. This type of BCC may be treated in a variety of ways.
Solid or Nodular BCC
A common type of BCC where the BCC Cells form in a large clump (or clumps). There may be small spaces called lacunae made up of debris from old cells. Surgical excision with a defined margin is all that is required because this type of BCC is well defined with clear margins – low chance of recurrence.
Cystic BCC
A rare type of BCC where the majority of the BCC is made up of cysts (unlike the small cysts found commonly in a solid BCC). Surgical excision with a defined margin is all that is required.
Basosquamous BCC
BCC with some features of an SCC (Squamous Cell Carcinoma).
Pigmented BCC
BCC that is pigmented. The pigmentation may also be seen clinically (prior to excision). The pigmented BCC is really a description and most pigmented BCC is nodular but may be found in all other types except perhaps morphoeic.
Morphoeic BCC
Morphoeic BCC pathologically corresponds to the clinical feature although the final diagnosis is made by examination of the pathological specimen.
The BCC cells are found in cords or strands within a network of tissue containing collagen (which makes the lesion feel firm). These cords off may be very thin (eg. 2-3 cells in thickness) and so the BCC may spread beyond what can be seen with the naked eye. Therefore, this type of BCC may require additional surgery.
Micronodular BCC
Micronodular BCC consists of multiple small nodules of BCC cells – unlike a solid BCC where there is a single of few larger nodules. The nodules of micronodular BCC may be found deeper in the dermis.
There may be gaps of normal skin in-between the small nodules s of micronodular BCC so it can be difficult to determine the precise edge of the BCC. Therefore this type of BCC may require monitoring or additional surgery and/or wider margins.
Infiltrating BCC
Infiltrating BCC consist of long strands of BCC cells that may be very thin eg just 2-3 cells thick. . They share quite a lot in common with morphoeic BCC except that the infiltrating BCC may extend deeply in the dermis and also extend fairly widely, often surrounded by collagen.
The tumour edges may be difficult to determine because they are less well defined – you can’t see the edge of the BCC as well. This type of BCC may require monitoring or additional surgery with wider margins.
What Terms might I see in a BCC Pathology Report?
The following Terminology might be seen in a BCC Pathology Report.
Palisading
The BCC Cells form in clumps or clusters, and they are a blue colour on the stain.
The BCC cells may be lined up at the edge of the BCC cells almost like bricks. This is referred to as Palisading.
Clefting
Clefting refers to “spaces” that appear (under the microscope) around some areas of BCC.
Basal Cell cancer cells
The Basal Cell Cancer Cells are blue in colour under the standard pathology stain.
Mitoses
The nuclei of the BCC Cells may show mitoses ie. cell division. They reflect the rate of cell division.
Apoptosis
Some of the BCC Cells die – which keeps the BCC in check. These cells appear pink in colour and this programmed cell death is referred to as apoptosis.
Perineural Invasion
The BCC cells may invade the cells – this is called perineural invasion and indicates a more aggressive BCC that may require additional monitoring and/or surgery.
BCC accounts for around 70% of skin cancers.
 ©South East Skin Clinic, All rights reserved
©South East Skin Clinic, All rights reserved
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}